Platelet-Rich Fibrin (PRF) has become one of the most widely used autologous regenerative therapies in dentistry, oral surgery, implantology, periodontics, and aesthetic medicine. By utilizing the patient’s own blood, PRF provides a concentrated source of platelets, leukocytes, cytokines, and growth factors that support tissue repair and regeneration without introducing synthetic materials or pharmaceuticals.
As PRF technology has evolved, clinicians now have access to multiple forms of PRF, including traditional solid PRF membranes and injectable liquid PRF (i-PRF). While both originate from the same blood sample, they differ significantly in preparation, fibrin architecture, handling characteristics, biological behavior, and clinical applications.
For dentists, implant specialists, aesthetic practitioners, and distributors evaluating PRF systems, understanding the differences between liquid PRF and solid PRF is essential for selecting the appropriate centrifugation protocol and collection tube. The final regenerative product depends not only on centrifuge settings but also on the tube used during preparation.
Liquid PRF Vs Solid PRF: Understanding the Difference Between
Both liquid PRF and solid PRF are derived from whole blood without extensive laboratory processing. Unlike Platelet-Rich Plasma (PRP), which relies on chemical anticoagulants to prevent clotting during centrifugation, PRF utilizes the body’s natural coagulation process to create a biologically active fibrin matrix capable of gradually releasing growth factors.
The primary difference lies in the stage of fibrin polymerization at the time of collection.
Liquid PRF (i-PRF) remains in a fluid state immediately after centrifugation. Because fibrin formation has been delayed, clinicians can inject the material directly into tissues or combine it with bone graft materials before polymerization occurs. Once applied, the fibrin network forms naturally within the treatment area.
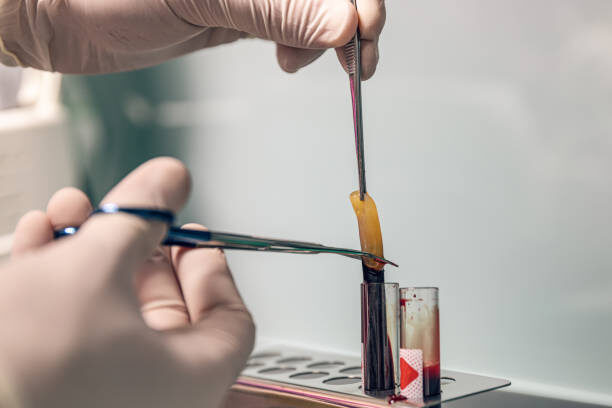
Solid PRF, on the other hand, forms a stable fibrin clot during centrifugation. The clot can be compressed into a membrane or plug that functions as a biologic scaffold. This structure provides both regenerative signaling and physical support for tissue healing.
In dentistry, the most commonly used solid form is Leukocyte- and Platelet-Rich Fibrin (L-PRF), which creates a dense fibrin membrane particularly suitable for surgical procedures and guided tissue regeneration.
Although both products contain platelets, leukocytes, and growth factors, their clinical applications and biological behavior differ substantially.

Liquid PRF vs. Solid PRF: Key Differences at a Glance
| Physical Form | Injectable liquid | Membrane or fibrin clot |
| Centrifugation Protocol | Low-speed, short-duration | Standard-speed clot formation |
| Fibrin Structure | Loose and developing | Dense and organized |
| Growth Factor Release | Faster initial release | Sustained release over time |
| Main Applications | Facial aesthetics, hair restoration, sticky bone | Wound healing, implant surgery, extraction sockets |
| Injectable | Yes | No |
| Bone Graft Mixing | Excellent | Limited |
| Membrane Function | Not applicable | Excellent |
| Surgical Site Coverage | Limited | Excellent |
| Handling Characteristics | Injectable and flowable | Structural and supportive |
Rather than competing technologies, these two forms of PRF address different clinical needs and often complement each other during the same procedure.
How Centrifugation Speed Influences PRF Structure
One of the most important variables affecting PRF quality is centrifugation speed and relative centrifugal force (RCF).
Modern PRF preparation increasingly follows the concept known as the Low-Speed Centrifugation Concept (LSCC). This approach aims to preserve a greater number of platelets, leukocytes, and regenerative cells within the fibrin matrix.
Higher centrifugation speeds generally:
- Produce denser fibrin networks
- Push more cellular components toward the bottom of the tube
- Reduce the number of regenerative cells retained in the upper plasma fraction
- Create firmer and more compact PRF clots
Lower centrifugation speeds typically:
- Retain more platelets and leukocytes
- Generate a looser fibrin architecture
- Increase cellular content within the final product
- Improve the injectable characteristics required for liquid PRF
Injectable PRF protocols typically use significantly lower centrifugal forces and shorter spin times than traditional PRF membrane protocols. This allows clinicians to collect the regenerative plasma fraction before extensive fibrin polymerization occurs.
Solid PRF protocols utilize centrifugation settings that encourage clot formation and fibrin organization. The resulting membrane exhibits greater structural integrity and can be manipulated during surgical procedures.
The fibrin architecture created during centrifugation directly influences growth factor release kinetics. A dense fibrin network typically functions as a biological reservoir, gradually releasing growth factors over a period of approximately 7–14 days. In contrast, liquid PRF often provides a stronger initial release of regenerative molecules shortly after application.
For this reason, centrifugation settings must be carefully matched to the intended clinical application.
Solid PRF Membranes: Best for Surgical Healing and Tissue Regeneration
Solid PRF remains the most widely used form of PRF in dentistry and oral surgery because it functions as both a biologic stimulant and a physical scaffold.
After centrifugation, clinicians remove the fibrin clot and often compress it into a membrane. This membrane can then be placed directly into or over the surgical site.
Common clinical applications include:
Tooth Extraction Sites
Following extraction, PRF membranes can be placed into the socket to support soft tissue healing, reduce postoperative discomfort, and help preserve alveolar bone volume.
Implant Dentistry
Many implant surgeons use PRF membranes around implant sites to support osseointegration and improve peri-implant soft tissue healing.
Guided Bone Regeneration (GBR)
When combined with bone graft materials, PRF membranes help stabilize the graft while delivering growth factors directly to the regenerative site.
Periodontal Surgery
PRF membranes are frequently used in gingival recession treatment, periodontal defect repair, and soft tissue grafting procedures.
Oral and Maxillofacial Surgery
The membrane structure makes PRF particularly valuable for larger surgical wounds where both biologic stimulation and tissue coverage are required.
The primary advantage of solid PRF is its three-dimensional fibrin scaffold. This structure supports cell migration, angiogenesis, tissue remodeling, and sustained growth factor release throughout the healing process.
For clinicians focused on wound healing and regenerative surgery, solid PRF often remains the preferred option.
Liquid PRF: Best for Injectable Regeneration and Facial Aesthetics
Injectable PRF (i-PRF) has rapidly gained popularity in aesthetic medicine and minimally invasive regenerative therapies.
Because the material remains fluid immediately after preparation, practitioners can inject it directly into target tissues before fibrin polymerization occurs.
Common applications include:
Facial Rejuvenation
Aesthetic practitioners frequently use liquid PRF to improve skin quality, texture, elasticity, and overall appearance. Growth factors released from platelets may stimulate collagen production and tissue regeneration.
Hair Restoration
i-PRF has become increasingly popular in hair restoration protocols designed to support hair follicle function and improve hair density.
Combination with Microneedling
Many clinics combine injectable PRF with microneedling procedures to enhance regenerative activity and accelerate recovery.
Injectable Regenerative Dentistry
Some clinicians utilize liquid PRF around implant sites and soft tissue defects where direct injection offers advantages over membrane placement.
Sticky Bone Preparation
One of the most important applications in implant dentistry involves combining liquid PRF with particulate bone graft materials.
As fibrin polymerizes, the graft particles become incorporated into a cohesive structure commonly known as sticky bone. This material improves handling characteristics, increases graft stability, and simplifies surgical placement.
The greatest advantage of liquid PRF is versatility. Its injectable nature allows clinicians to deliver regenerative factors precisely where they are needed, including areas inaccessible to traditional membranes.

How Tube Choice Determines Whether You Obtain Liquid or Solid PRF
Many clinicians focus primarily on centrifuge settings while overlooking an equally important factor: the collection tube.
Tube composition directly influences coagulation timing, fibrin formation, cellular retention, and the overall quality of the final PRF product.
Tubes for Solid PRF
Traditional solid PRF preparation has historically utilized glass tubes or silica-coated plastic tubes.
The hydrophilic surface of glass and silica can activate the intrinsic coagulation pathway through Factor XII activation, encouraging rapid fibrin polymerization and clot formation during centrifugation.
However, as PRF protocols continue to evolve, many clinicians increasingly prefer additive-free PRF tubes designed to avoid introducing foreign particles into the fibrin matrix while still supporting reliable clot formation.
High-quality PRF tubes for membrane production should provide:
- Consistent vacuum levels
- Biocompatible tube surfaces
- Uniform clot formation
- Reliable platelet capture
- Minimal contamination risk
- Reproducible clinical outcomes
Tubes for Liquid PRF
Liquid PRF preparation generally requires additive-free hydrophobic plastic tubes, commonly manufactured from medical-grade PET.
Because hydrophobic PET surfaces do not immediately activate the intrinsic clotting cascade, coagulation occurs more slowly. This provides a working window during which clinicians can collect and inject the liquid PRF before fibrin polymerization is completed.
When evaluating i-PRF systems, clinicians and distributors should examine:
- Tube material composition
- Vacuum accuracy
- Sterility assurance
- Manufacturing consistency
- Protocol compatibility
- Batch-to-batch reliability
Even minor variations in tube design can influence separation quality, clot formation, growth factor concentration, and clinical reproducibility.
For this reason, experienced practitioners often standardize both their centrifugation protocols and tube suppliers to achieve consistent regenerative outcomes.
Liquid PRF Vs Solid PRF: Which Form Is Better?
The answer depends entirely on the clinical objective.
If the goal is extraction socket preservation, implant surgery, guided bone regeneration, periodontal procedures, or surgical wound coverage, solid PRF membranes generally provide the greatest benefit because of their structural properties and prolonged growth factor release.
If the objective involves facial aesthetics, hair restoration, injectable regenerative therapy, or sticky bone preparation, liquid PRF often offers greater flexibility and precision.
Many advanced clinics now utilize both forms during the same procedure. For example, an implant surgeon may prepare liquid PRF to create sticky bone while simultaneously producing solid PRF membranes for graft coverage and wound protection.
Rather than viewing liquid PRF and solid PRF as competing technologies, clinicians increasingly recognize them as complementary tools within a comprehensive regenerative treatment strategy.
Whether your practice focuses on implant dentistry, oral surgery, facial aesthetics, or hair restoration, selecting the correct PRF tube is essential for achieving consistent regenerative outcomes. High-quality PRF collection tubes, combined with validated centrifugation protocols, help ensure predictable fibrin formation, optimal growth factor preservation, and reproducible clinical results.
For distributors and clinics evaluating PRF systems, understanding the relationship between centrifugation parameters, tube design, and final PRF form is the key to selecting the most appropriate solution for every treatment indication.
FAQs for Liquid PRF Vs Solid PRF
Is liquid PRF stronger than solid PRF?
Not necessarily. Both contain valuable growth factors and regenerative cells. Liquid PRF is ideal for injection and graft mixing, while solid PRF provides structural support and prolonged growth factor release.
Can one blood draw produce both liquid PRF and solid PRF?
Yes. Many clinicians collect multiple tubes and process them using different centrifugation protocols to obtain both injectable PRF and PRF membranes during the same treatment session.
Why does centrifugation speed matter in PRF preparation?
Centrifugation speed influences cell distribution, fibrin density, growth factor release patterns, and the physical characteristics of the final PRF product.
What is sticky bone?
Sticky bone is created by combining liquid PRF with particulate bone graft material. As fibrin polymerizes, it binds graft particles together into a stable, easy-to-handle regenerative matrix.
Can the wrong tube affect PRF quality?
Yes. Tube material, surface properties, vacuum consistency, and manufacturing quality can significantly influence clot formation, cellular retention, fibrin architecture, and overall treatment reproducibility.
Which PRF form is most commonly used in dentistry?
Solid PRF membranes remain the most widely used form in surgical dentistry, implantology, and periodontal procedures. However, liquid PRF continues to gain popularity for sticky bone preparation and minimally invasive regenerative treatments.